Tags
- accounting
- administration
- Ambulatory Surgical Center
- anesthesia
- anesthesia residency
- anesthesiologist
- anesthesiology
- ASC
- board of directors
- board of directors data analysis
- business
- CEO
- cfo
- chairman
- cmo
- concept graph
- concept map
- constraints
- constraint theory
- COO
- cost accounting
- CRNA
- decisio
- decision algorithm
- deparment chairman
- dissatisfaction
- emotional intelligence
- finance
- flipping
- flip room
- FTE
- fungibility
- healthcare reform
- healthcare systems analysis
- healthcare systems engineering
- hospital
- hospital patient flow
- incentives
- information technology
- legal risk
- nurses
- operating room
- operating room efficiency
- operating room productivity
- operating theatre
- operations m
- operations management
- OR
- OR scheduling
- OR throughput
- PACU
- preOP
- revenue sharing
- risk
- risk management
- room flipping
- satisfaction
- schedule
- scheduling
- spc
- sqc
- surge
- surgeon
- surgery
- surgical case
- systems analysis
- systems engineering
- theory of constraints
- throughput
- throughput accounting
- toc
- TOT
- turn over time
- vice chairman
Category Archives: CEO
Finance Leaders Bemoan Talent Shortage
http://www3.cfo.com/article/2013/4/training_finance-function-training-skills-talent-corporate-executive-board-kruti-bharucha?utm_source=taboola Read the comments in the article.
Posted in Accounting, CEO, healthcare reform
Leave a comment
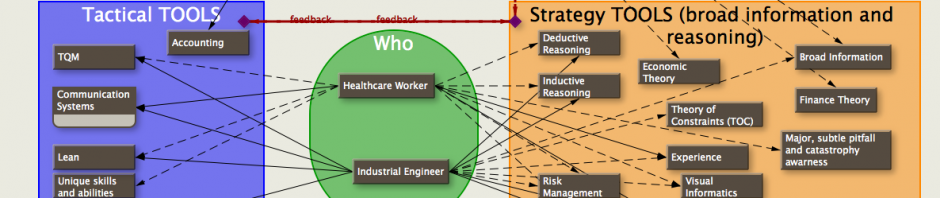
Can engineers and physicians mix…from LinkedIn conversation
Follow David Can engineers and physicians mix? When doing and hearing about healthcare performance improvement it seems much is dependent on doctors and engineers collaborating. Yet this is difficult. Sometimes impossible when implementing. Are they too different to succeed? 7 … Continue reading
Posted in CEO, experts, healthcare reform, Uncategorized
Tagged CEO, COO, healthcares systems engineering, systems engineering
Leave a comment
TA (throughput accounting) and TDABC (time driven activity based costing)….the fabric, the ‘warp and woof’ of healthcare accounting?
also see: throughput accounting…a natural for hospitals? Linkedin thread also see: throughput accounting (TA) vs activity based costing (ABC) also see: FTE vs cost accounting… when PUNs equal CUEs also see: When you’re lost, use a map… also see: Graphic Simulation … Continue reading
Linkedin converstion: “How will medical tourism insert itself into mainstream of US healthcare reform?”
MariaUnfollow How will medical tourism insert itself into the mainstream of U.S. healthcare reform? Under healthcare reform, employers are beginning to express interest in concepts and reform measures which have variously been labeled ―value-based, ―results-based, ―performance-based, or ―outcomes-based purchasing and … Continue reading
Posted in ASC, board of directors, CEO, healthcare reform
Tagged medical tourism; healthcare reform
Leave a comment
Linkedin Medical Tourism excerpt: Major Diagnostic Category flaws
Medical Tourism for Group Health: Using Major Diagnostic Categories (MDCs) to Predict Medical Tourism Utilization – A Flawed Strategy that Can Lead to Unrealistic Expectations The MDC is a very commonly used term, and widely misunderstood. All diagnoses or illnesses … Continue reading
Is Healthcare’s Insular Culture a Liability or Benefit? Linkedin thread started by Peter Hadras…
Is Healthcare’s Insular Culture a Liability or Benefit? Working recently in the healthcare industry, I keep being struck by the deep-seated culture that unless the solution or practitioner is from healthcare, then it cannot be applied to a solve a … Continue reading
Posted in board of directors, CEO, Uncategorized
Leave a comment
throughput accounting…a natural for hospitals? Linkedin thread.
see also: TA (throughput accounting) and TDABC (time driven activity based costing)…the fabric, the ‘warp and woof’ of healthcare accounting? Throughput Accounting— a natural for Hospitals? In my work with increasing OR productivity, throughput accounting quickly shows the benefits of … Continue reading
bad research…or bad reporting?
This is an example of the perils (morbidity, mortality, and financial) of mathematical manipulation of data by researchers in basing broad conclusions without more fully understanding the processes and externalities involved: Unnecessary anesthesia adds $1B to health spending – FierceHealthcare … Continue reading
Posted in Accounting, Ambulatory Surgical Center, anesthesiologist, ASC, board of directors, CEO, surgeon
Tagged anesthesia, OR scheduling, OR throughput, risk, risk management, scheduling
Leave a comment
throughput accounting (TA) vs activity based costing (abc)…
see also: TA (throughput accounting) and TDABC (time driven activity based costing)…the fabric, the ‘warp and woof’ of healthcare accounting? from a Linkedin topic: Just thought I’d expand on some thoughts about Acitivity Based Costing (ABC) vs Thoughput Accounting (TPA): … Continue reading
Posted in Accounting, CEO, healthcare reform
Tagged accounting, cfo, COO, cost accounting, toc
Leave a comment
accounting and scheduling come together…
It took a few days (alright… quite a few days), but now my accounting software (great company-versatile software) collects accounting data in the standard cost accounting manner, yet reports it in a Throughput Accounting or Activity-based Accounting way so that … Continue reading
Posted in Accounting, anesthesiologist, ASC, CEO, healthcare reform, scheduling
Leave a comment
Healthcare Administrator-Physician divide
The following is an excerpt from an ongoing discussion in the Linkedin group ‘Healthcare Executives Network’. It broaches several problems and approaches that are necessary to understand before finding workable solutions, and could be taken as a preface for a … Continue reading
Posted in CEO, Uncategorized
Tagged CEO, healthcare, healthcare systems engineering, physicians
Leave a comment
FTE, utilization, and cost accounting … when PUNs equal CUEs
also see: Graph of CRNA usage for optimized Surgeon Schedule also see: TA(throughput accounting) and TDABC (time driven activity based costing)….the fabric, the ‘warp and woof’ of healthcare — Cost accounting (whether standard costing or TDABC) is based on the concept … Continue reading
Posted in Ambulatory Surgical Center, anesthesiologist, CEO, healthcare reform, scheduling, surgeon, Uncategorized
Tagged anesthesiology, cfo, COO, cost accounting, FTE, full time employee
1 Comment
a box lunch to go…
It looks as though healthcare funding will be cut shortly. Medicare will be on the chopping block soon, reimbursements for hospitals will be down. Those who don’t think outside the box–who never saw the lid of the box closing–will be … Continue reading
Posted in board of directors, CEO, healthcare reform
Tagged CEO, constraints, COO, healthcare reform
Leave a comment
Do Doctors run Hospitals better?
internet: http://ftp.iza.org/dp5830.pdf local: Who Needs an MBA So which is better, an MD, MBA, or MD / MBA?
the dark side of hospital patient flow… Part 1
Flow is defined as the quantity of some item (units of an item) passing by, leaving, or arriving at some point in a designated unit of time. So, flow is defined by four parameters: units(1) of an item(1) , a … Continue reading
Posted in board of directors, CEO, healthcare reform, scheduling, surgeon
Tagged CEO, cfo, COO, hospital patient flow
1 Comment
getting your hands dirty…
Sometimes, to get what you want, you have to jump in and get your hands dirty… It’s been a month since my last post, a series of posts dealing with ‘what ifs’ and some simple simulations dealing with scheduling OR … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, Uncategorized
Tagged cfo, healthcare reform, healthcare systems analysis, OR, scheduling
Leave a comment
putting it all together…intra-case and inter-case….TOT and more
There are a thousand variations of the following examples, but I hope these four graphs will get across some ideas. For potential economic effects, see: Wasting $2.7 million dollars a year. Each of the following graphs has 5 bars. Each … Continue reading
Posted in anesthesiologist, board of directors, CEO, healthcare reform, scheduling, surgeon, Uncategorized
Tagged anesthesia, scheduling, surgeon, toc, TOT
Leave a comment
clinical resolution of systems engineering scheduling in the OR…
No new graphs today… Let’s discuss the resolution of a systems engineer in improving turnover time (TOT). In the last few blogs I showed the difference in TOT due solely to who sees the patient in the pre-op holding area, … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesiology, CEO, COO, healthcare systems analysis, nurses, scheduling, surgeon, surgery
Leave a comment
Big Bwana and little bwana…
Everything in the below graph is adjustable (and is derived from less data than is normally collected in an OR). It’s quite useful when deciding how to create your portfolio of surgeons, anesthesiologists, or nurses to limit the short-comings, and … Continue reading
Posted in anesthesiologist, board of directors, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, COO, finance, healthcare reform, healthcare systems analysis, OR, surgery, surgical case
Leave a comment
the cost of late surgeons… and the revenue from early surgeons
The purple bars represent the time saved for nursing staff and anesthesia if there is a policy for the surgeon to be ready to cut 30 minutes (adjustable) before the scheduled start of cases in the morning. The effects of … Continue reading
Typical OR case dissected with details…
These are the relevant milestones and intervals in a typical OR case. I left off the details so as not to detract from the comparison to the normal representation of an OR case as a single block of time with … Continue reading
Posted in anesthesiologist, board of directors, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, CEO, COO, healthcare reform, healthcare systems analysis, scheduling, surgery
Leave a comment
So much data…so little time
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged COO, healthcare reform, healthcare systems analysis, surgery, surgical case
Leave a comment
FT: “Chief profitability officers still rare”
The Financial Times has new articles emphasizing that the CFO needs to know more systems engineering, have better analytical skills, and understand IT better. Surprised? Chief probability officers still rare Competitive difference is in the analysis Finance heads need much … Continue reading
Posted in board of directors, CEO, healthcare reform
Tagged board of directors, CEO, cfo, COO, healthcare reform, healthcare systems analysis
Leave a comment
FT: “Competitive difference is in the Analysis”
I’ve been discussing this, and showing examples, on my weblog for some time. Here’s a (The) major financial newspaper saying the same thing: Competitive difference is in the analysis
Posted in board of directors, CEO, healthcare reform
Tagged CEO, cfo, COO, healthcare reform, healthcare systems analysis, systems analysis
Leave a comment
FT: “Finance heads need much wider view of IT”
For those of you who won’t subscribe to Financial Times… Finance heads need much wider view of IT The Financial Times is a premier newspaper dedicated to the finance world: CFOs, CEOs, CFAs. If you pass the article along, a … Continue reading
Posted in board of directors, CEO, healthcare reform
Tagged board of directors, CEO, cfo, COO, healthcare reform, healthcare systems analysis
Leave a comment
new scheduler…timeline and map integration
Operating rooms are expensive assets; you don’t want them sitting idle when people need them. Each room may be equipped differently; you want to schedule procedures in the most appropriate room. To complicate matters, some procedures require special equipment that … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, CEO, COO, scheduling, surgery
Leave a comment
board can struggle with data puzzle…
Board can Struggle with Data Analysis I’ve discussed visual analytics before, and its ability to bring actionable information to both the CEO and worker on the floor. The Financial Times has just published the above Special Report saying that boards … Continue reading
non-expert decison making: perils of democracy…
When making an individual decision, or whether voting as a group, the ‘strength’ of one’s conviction on a topic should be modified by one’s expertise before coming to a final resolution. All decisions have pros and cons, all of different … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, surgeon
Tagged anesthesia, CEO, COO, CRNA, decision algorithm, surgeon
Leave a comment
hold the mayo…
Unfortunately, I forgot to take a picture of my poster presentation at the Mayo Clinic’s 3rd Annual Healthcare Systems Engineering meeting. However, I did take a picture as I was putting it together the week before. Here it is, in … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, COO, scheduling, surgeon
Leave a comment
business interest…
When we started this blog, we didn’t know how well it would be received. Even though there were few comments, we could follow how many viewers had dropped by to have a look and download our graphs and articles. We … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged CEO, COO, healthcare reform
Leave a comment
Protected: theory, tools, and techniques… abstract
There is no excerpt because this is a protected post.
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, COO, finance, surgeon, throughput
Enter your password to view comments.
the law of unintended consequences…staffing anesthesiologists
Value: easily and potentially > than $1,000,000 a year Let’s suppose that a hospital wants fellowship trained anesthesiologists to do all their cases: pediatric anesthesia fellowship for all pediatric cases, neuroanesthesia fellowship for all neuro cases, ob-gyn fellowship for all … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling
Tagged anesthesia, CEO, cfo, COO, legal risk, risk, risk management
2 Comments
Conflict of interests for surgeons?…
I’ve seen this potential for abuse over the years. It’s probably just jealousy on my part… we get donuts from the reps, some of the surgeons get all expense paid trips to exotic (well, sometimes exotic) locations. There may be … Continue reading
Posted in CEO, healthcare reform, surgeon
Tagged CEO, finance, healthcare reform, surgeon
Leave a comment
Operations-a-Finance….cost accounting vs managerial accounting vs others
“If discussing shop with a Finance person, one thought is to get a feel of where they are coming from. How difficult is it to get them to use “GAAP” in the conversation and what is their attitude about it?” … Continue reading
Posted in CEO, healthcare reform
Tagged CEO, finance, healthcare reform, operations management
Leave a comment
Protected: Concerning hospitals hiring physicians…
There is no excerpt because this is a protected post.
Posted in CEO, healthcare reform
Enter your password to view comments.
only the beginning…
In my last year of anesthesia residency, an attending told the graduating class “You’re just beginning. We hope we’ve taught you enough so that you won’t kill anyone.” A surgical friend of mine said that he was very good technically … Continue reading
Fiscally responsible OR expansion…
This post is in response to a question posted in the Yahoo group (hme) about ‘triggers’ for OR room/suite expansion. As usual, in healthcare, nothing is easy: The decision to increase the number of OR’s can’t be made solely on … Continue reading
Process control…
All the charts and graphs that you see in this blog are process control charts—like every efficient, productive industry (Boeing, GE, Toyota) uses. Every day, even during the day, you use these charts to see where processes need changes to … Continue reading
Disruptive behavior… zero tolerance by Joint Commission; Is your hospital in compliance?
Physician and nurse executives team up to fight disruptive behavior The American College of Physician Executives and the American Organization of Nurse Executives are joining forces to stamp out disruptive behavior. The two organizations are providing resources and guidance to … Continue reading
Tower of Babel…
One of the major anesthesia journals is still publishing articles on the financial benefits of using shorter acting drugs for anesthesia. Anyone with two neurons and a synapse who practices anesthesia has known this for over a decade. When will … Continue reading
Let sleeping children lie…
While I was at KFSH&RC in Saudi Arabia, a Kiwi friend of mine who was head of the radiation oncology department asked me if my department (anesthesia) could help them expedite their pediatric radiation treatments. It would take them all … Continue reading
‘When Worlds Collide’…. Finance and Healthcare
There’s an insightful book authored by the current CEO and co-COO of Pimco (also past investment manager of Harvard Management Company, Harvard University) Mohamed A. El-Erian called ‘When Markets Collide–Investment Strategies for the Age of Global Economic Change’. The book … Continue reading
“PowerPoint is evil”
In a prior post I made the statement that cost accounting was EVIL. This recent article about Dr. Edward Tufte’s (Professor Emeritus of Political Science, Statistics and Computer Science at Yale University) appointment to a post in the Obama administration … Continue reading
Posted in CEO, healthcare reform
Leave a comment
When you’re lost, use a map…
see also: TA(throughput accounting) and TDABC (time driven activity based costing)…the fabric, the ‘warp and woof’ of healthcare accounting? I had a brief, but interesting conversation with a CMO of a large hospital recently. To his credit, he’s trying to … Continue reading
How to Tell the Productive Surgeons from the non-Productive
The previous blogs were concerned with economic gains for the different parties (surgeon, anesthesia, hospital) by optimizing the relationship each case had with another case (inter-case) — the OR schedule. Each OR is dramatically different, and what works for one … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesia, CEO, linkedin, risk management, schedule, scheduling, surgeon
2 Comments
the fungible anesthetist…
See also: staffing anesthesiologists…the law of unintended consequences I’m emphasizing anesthetists as the fungible commodity (since they can be more readily fungible, and expensive), however it could be anything such as nurses, surgeons, equipment, OR rooms, etc. The existence of similar … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, COO, schedule, scheduling, surgeon
1 Comment
Same as last post. CRNA centric view of schedule for the day.
Here’s a different view of CRNA usage (bottom graph of last post –January 23, 2010). It’s organized by CRNA—Follow the CRNA through the day to successive rooms. The CRNA (1aa, 1ab, 1af…) is listed to the right of every horizontal … Continue reading
Posted in anesthesiologist, CEO, scheduling
Tagged anesthesiologist, CEO, COO, CRNA, schedule, scheduling
Leave a comment
The bottom line…
Each row represents an individual CRNA. If over half of each time unit (10 minutes) is billable on an anesthesia record, then it is red. Less than half is yellow. Exactly half is green. Lines that are all yellow belong … Continue reading
Posted in anesthesiologist, CEO, scheduling
Tagged anesthesiologist, schedule, scheduling
Leave a comment
Can I trust my state medicaid and medicare system?
Missouri, one of only 3 states to receive an “A” in management information by Governing Magazine in 2008 is highlighted in the following article. If Missouri is in the top 3, how can we trust the rest? Best to have … Continue reading
Posted in anesthesiologist, CEO, surgeon
Tagged administration, anesthesiologist, CEO, finance, surgeon
Leave a comment
Graphs of Actual and Optimized Surgical Schedule
Warning! Not for the graphically challenged. In reference to the graphs I posted on January 14, 2010, I’ve added several graphs with detailed information. The first graph is of the actual room schedule (non-optimized) before optimizing it by a better … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, COO, linkedin, schedule, scheduling, surgeon
1 Comment
I don’t understand what you mean…
We were having a discussion the other day about whether it would be more profitable to teach finance concepts to the people doing the actual work on the shop floor (‘workers’) or to teach the finance and accounting people (‘suits’) … Continue reading
I love my work, but…
As a follow-up from my post on Jan 14, 2010 “Are you wasting your surgeons’ time?” showing how surgeons can decrease their time in the OR, here’s a recent article from the Center for Healthcare Policy and Research and Department … Continue reading
Posted in CEO, scheduling, surgeon
Tagged CEO, dissatisfaction, satisfaction, schedule, scheduling, surgeon
Leave a comment
Who’s in charge here, anyway?
A big problem in the OR is that not everyone is working for the same goal. The major players are surgeons, anesthesiologists, and the hospital (nurses, orderlies, administrators, etc.), each wanting to maximize their income and minimize their work and … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, schedule, scheduling, surgeon
Leave a comment
With whom should I do my cases?
<click on the above graph for a larger image> The above graph is an example of finished data analysis for three different orthopedic groups (Arizona Cutters, ORO Pods, Tucson Bones) which are deciding in which hospital, and with which anesthesia … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, finance, linkedin, schedule, scheduling, surgeon
Leave a comment
