Tags
- accounting
- administration
- Ambulatory Surgical Center
- anesthesia
- anesthesia residency
- anesthesiologist
- anesthesiology
- ASC
- board of directors
- board of directors data analysis
- business
- CEO
- cfo
- chairman
- cmo
- concept graph
- concept map
- constraints
- constraint theory
- COO
- cost accounting
- CRNA
- decisio
- decision algorithm
- deparment chairman
- dissatisfaction
- emotional intelligence
- finance
- flipping
- flip room
- FTE
- fungibility
- healthcare reform
- healthcare systems analysis
- healthcare systems engineering
- hospital
- hospital patient flow
- incentives
- information technology
- legal risk
- nurses
- operating room
- operating room efficiency
- operating room productivity
- operating theatre
- operations m
- operations management
- OR
- OR scheduling
- OR throughput
- PACU
- preOP
- revenue sharing
- risk
- risk management
- room flipping
- satisfaction
- schedule
- scheduling
- spc
- sqc
- surge
- surgeon
- surgery
- surgical case
- systems analysis
- systems engineering
- theory of constraints
- throughput
- throughput accounting
- toc
- TOT
- turn over time
- vice chairman
Tag Archives: scheduling
What is the cost of a minute of intra-unit patient transport time….from LinkedIn conversation
Follow Brendan What is the cost of a minute of intra-unit patient transport time? The cost of a minute of time in patient transport is a questions we get asked quite often by acute care leaders. Is anyone aware of … Continue reading
constraint theory and Pareto Optimals…
Brian Gregory, MD, MBA • Wayne, good question. Healthcare is a funny animal–you have constraints within constraints. One of the main tenets of ToC is to pick what you want to be the constraint. In the case of the OR (ER, radiology, … Continue reading
bad research…or bad reporting?
This is an example of the perils (morbidity, mortality, and financial) of mathematical manipulation of data by researchers in basing broad conclusions without more fully understanding the processes and externalities involved: Unnecessary anesthesia adds $1B to health spending – FierceHealthcare … Continue reading
Posted in Accounting, Ambulatory Surgical Center, anesthesiologist, ASC, board of directors, CEO, surgeon
Tagged anesthesia, OR scheduling, OR throughput, risk, risk management, scheduling
Leave a comment
increase strategy to increase throughput: …data in context…lean in context…flipped rooms…
Why is this important? It can significantly increase total throughput and throughput as referenced by a particular agent (surgeon, anesthesiologist, hospital). Increased throughput can be converted into large increases in revenue. It can decrease cost for all agents. It can … Continue reading
Posted in Ambulatory Surgical Center, anesthesiologist, ASC, scheduling, surgeon
Tagged anesthesia, CEO, COO, OR scheduling, room flipping, scheduling, surgeon
Leave a comment
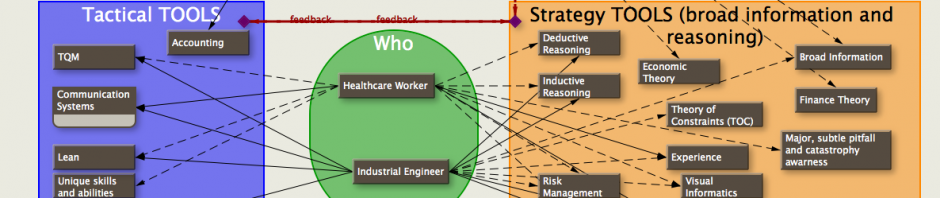
OR scheduling concept map (concept diagram)…
A few years ago I diagrammed several concepts involved in scheduling an OR onto this graph. The intent was to take advantage (or nullify disadvantages) of characteristics of individual surgeons and anesthetists. The interplay of these concepts and individual factors … Continue reading
Posted in anesthesiologist, concept graph, concept map, healthcare reform, scheduling, surgeon
Tagged anesthesia, concept graph, concept map, COO, OR, scheduling, surgery
2 Comments
getting your hands dirty…
Sometimes, to get what you want, you have to jump in and get your hands dirty… It’s been a month since my last post, a series of posts dealing with ‘what ifs’ and some simple simulations dealing with scheduling OR … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, Uncategorized
Tagged cfo, healthcare reform, healthcare systems analysis, OR, scheduling
Leave a comment
putting it all together…intra-case and inter-case….TOT and more
There are a thousand variations of the following examples, but I hope these four graphs will get across some ideas. For potential economic effects, see: Wasting $2.7 million dollars a year. Each of the following graphs has 5 bars. Each … Continue reading
Posted in anesthesiologist, board of directors, CEO, healthcare reform, scheduling, surgeon, Uncategorized
Tagged anesthesia, scheduling, surgeon, toc, TOT
Leave a comment
clinical resolution of systems engineering scheduling in the OR…
No new graphs today… Let’s discuss the resolution of a systems engineer in improving turnover time (TOT). In the last few blogs I showed the difference in TOT due solely to who sees the patient in the pre-op holding area, … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesiology, CEO, COO, healthcare systems analysis, nurses, scheduling, surgeon, surgery
Leave a comment
coffee and donuts…. time for a break
Oh what fun… This is just one of many factors affecting turnover time (TOT). For the sake of smaller graphs and clarity, I’m showing only the times till anesthesia induces the patient to show the comparison of … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesiology, OR, scheduling, theory of constraints
2 Comments
difficulties with start times and TOT in the OR…
The following are excerpts from a discussion concerning Turn-Around-Time (TOT) in the OR. They relate to my recent posts on scheduling, and show the complexity/difficulty in defining the problems and solving them: ____ she: There are benchmarks out in the … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, decisio, OR, scheduling, surgical case
Leave a comment
micro real options in the OR…
One advantage of performing virtually identical cases—such as specialty ORs (cataract surgery would be an example) is that the room setup is virtually identical and a great deal of time can be saved (or avoided) by being able to put … Continue reading
Posted in anesthesiologist, healthcare reform, scheduling, surgeon
Tagged COO, finance, OR, schedule, scheduling
Leave a comment
the surgeon as a constraint…
This graph shows components of surgical time during a typical surgical case: red bar: primary surgeon needs to be present and is present top yellow bar: surgeon needs to be present, but isn’t–he’s late and everyone is waiting … Continue reading
Posted in healthcare reform, scheduling, surgeon
Tagged constraints, COO, healthcare reform, healthcare systems analysis, scheduling, surgeon
Leave a comment
Typical OR case dissected with details…
These are the relevant milestones and intervals in a typical OR case. I left off the details so as not to detract from the comparison to the normal representation of an OR case as a single block of time with … Continue reading
Posted in anesthesiologist, board of directors, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, CEO, COO, healthcare reform, healthcare systems analysis, scheduling, surgery
Leave a comment
new scheduler…timeline and map integration
Operating rooms are expensive assets; you don’t want them sitting idle when people need them. Each room may be equipped differently; you want to schedule procedures in the most appropriate room. To complicate matters, some procedures require special equipment that … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, CEO, COO, scheduling, surgery
Leave a comment
new OR scheduler…
I’ve been experimenting with a new scheduler. There are many options for visually representing information about OR cases. The scheduler is easily adapted for collecting data to analyze later. The scheduler also has a map view that can include even … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, COO, scheduling, surgery
Leave a comment
sample new OR scheduler
For all those OR schedulers out there, here’s a new approach. I left most of the data off on purpose to emphasize the information that the graphics—lines, blocks, fonts, colors, sizes, and proximity— can show. When in the program, pages … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, COO, finance, schedule, scheduling, surge, throughput
Leave a comment
hold the mayo…
Unfortunately, I forgot to take a picture of my poster presentation at the Mayo Clinic’s 3rd Annual Healthcare Systems Engineering meeting. However, I did take a picture as I was putting it together the week before. Here it is, in … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, COO, scheduling, surgeon
Leave a comment
time to call it a day…
About two weeks ago, I returned after having honored a request from a Mayo researcher to give my poster presentation (a rational and extremely profitable OR scheduling and analysis system that I’ve actually used) at the Mayo Clinic’s 3rd Annual … Continue reading
OR throughput, flipping rooms with fast and slow anesthesia…
I found some graphs that I put together a couple of years ago. The results are born out empirically (at least by my experience in the OR). Lots of information about who to hire, who to fire, who to … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, COO, scheduling, surgeon
2 Comments
Fiscally responsible OR expansion…
This post is in response to a question posted in the Yahoo group (hme) about ‘triggers’ for OR room/suite expansion. As usual, in healthcare, nothing is easy: The decision to increase the number of OR’s can’t be made solely on … Continue reading
Geek humor…
On spaghetti and resource locking: A brief, yet helpful, lesson on elementary resource-locking strategy « The Reinvigorated Programmer
Let sleeping children lie…
While I was at KFSH&RC in Saudi Arabia, a Kiwi friend of mine who was head of the radiation oncology department asked me if my department (anesthesia) could help them expedite their pediatric radiation treatments. It would take them all … Continue reading
When you’re lost, use a map…
see also: TA(throughput accounting) and TDABC (time driven activity based costing)…the fabric, the ‘warp and woof’ of healthcare accounting? I had a brief, but interesting conversation with a CMO of a large hospital recently. To his credit, he’s trying to … Continue reading
How to Tell the Productive Surgeons from the non-Productive
The previous blogs were concerned with economic gains for the different parties (surgeon, anesthesia, hospital) by optimizing the relationship each case had with another case (inter-case) — the OR schedule. Each OR is dramatically different, and what works for one … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesia, CEO, linkedin, risk management, schedule, scheduling, surgeon
2 Comments
communication…life line
With today’s technologies, there are multiple ways for anesthesiologists and surgeons to keep organized and transfer documents while driving in the city, roaming the halls of the hospital, or during a case in the OR. No one should have to … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, anesthesiologist, schedule, scheduling, surgeon
Leave a comment
the fungible anesthetist…
See also: staffing anesthesiologists…the law of unintended consequences I’m emphasizing anesthetists as the fungible commodity (since they can be more readily fungible, and expensive), however it could be anything such as nurses, surgeons, equipment, OR rooms, etc. The existence of similar … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, COO, schedule, scheduling, surgeon
1 Comment
incentive, compensation, transparency
Incentive, Competitiveness, Transparency If most of anesthesiologists are supervising CRNAs, the anesthesiologists’ job is to increase the amount of the CRNAs’ billable time at the facility. Have the anesthesiologists do all the pre-ops, IVs in the pre-op area, and care … Continue reading
Posted in anesthesiologist, scheduling
Tagged anesthesiologist, CRNA, schedule, scheduling
Leave a comment
Same as last post. CRNA centric view of schedule for the day.
Here’s a different view of CRNA usage (bottom graph of last post –January 23, 2010). It’s organized by CRNA—Follow the CRNA through the day to successive rooms. The CRNA (1aa, 1ab, 1af…) is listed to the right of every horizontal … Continue reading
Posted in anesthesiologist, CEO, scheduling
Tagged anesthesiologist, CEO, COO, CRNA, schedule, scheduling
Leave a comment
The bottom line…
Each row represents an individual CRNA. If over half of each time unit (10 minutes) is billable on an anesthesia record, then it is red. Less than half is yellow. Exactly half is green. Lines that are all yellow belong … Continue reading
Posted in anesthesiologist, CEO, scheduling
Tagged anesthesiologist, schedule, scheduling
Leave a comment
Graph of CRNA usage for optimized Surgeon Schedule
also see: FTE vs cost accounting … when PUNs equal CUEs also see: Wasting surgeons’ time This is a graph of the CRNA usage for the Optimized Surgeon schedule from the blog post dated Jan 20, 2010. Compare this graph to … Continue reading
Posted in anesthesiologist, scheduling
Tagged anesthesiologist, CRNA, schedule, scheduling
1 Comment
Graphs of Actual and Optimized Surgical Schedule
Warning! Not for the graphically challenged. In reference to the graphs I posted on January 14, 2010, I’ve added several graphs with detailed information. The first graph is of the actual room schedule (non-optimized) before optimizing it by a better … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, COO, linkedin, schedule, scheduling, surgeon
1 Comment
I don’t understand what you mean…
We were having a discussion the other day about whether it would be more profitable to teach finance concepts to the people doing the actual work on the shop floor (‘workers’) or to teach the finance and accounting people (‘suits’) … Continue reading
I love my work, but…
As a follow-up from my post on Jan 14, 2010 “Are you wasting your surgeons’ time?” showing how surgeons can decrease their time in the OR, here’s a recent article from the Center for Healthcare Policy and Research and Department … Continue reading
Posted in CEO, scheduling, surgeon
Tagged CEO, dissatisfaction, satisfaction, schedule, scheduling, surgeon
Leave a comment
Who’s in charge here, anyway?
A big problem in the OR is that not everyone is working for the same goal. The major players are surgeons, anesthesiologists, and the hospital (nurses, orderlies, administrators, etc.), each wanting to maximize their income and minimize their work and … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, schedule, scheduling, surgeon
Leave a comment
With whom should I do my cases?
<click on the above graph for a larger image> The above graph is an example of finished data analysis for three different orthopedic groups (Arizona Cutters, ORO Pods, Tucson Bones) which are deciding in which hospital, and with which anesthesia … Continue reading
Posted in anesthesiologist, CEO, scheduling, surgeon
Tagged anesthesiologist, CEO, finance, linkedin, schedule, scheduling, surgeon
Leave a comment
Do you know where your CRNAs are?
<click on graph to enlarge in separate window> [Note that the scale for the upper and lower graphs are different] I mentioned in the prior post that my client had wanted an analysis of how well they were using their … Continue reading
Posted in anesthesiologist, scheduling
Tagged anesthesiologist, COO, CRNA, finance, schedule, scheduling
1 Comment
