
Distribution of total CRNA work hours for optimized surgeon schedule
also see: FTE vs cost accounting … when PUNs equal CUEs
also see: Wasting surgeons’ time
This is a graph of the CRNA usage for the Optimized Surgeon schedule from the blog post dated Jan 20, 2010. Compare this graph to the ones in the blog dated Jan 17, 2010 “Do you know where your CRNAs are?“. The total amount of actual working time for the CRNAs in this graph is 157 hrs instead of 147 hrs in the actual non-optimized graph, mostly because I rescheduled a 7 hr neurosurgical case from around midnight to earlier that day to see the effect of moving quasi-emergency cases that could have been accomplished earlier if there had been time available. In addition there will be some discrepancy because of variations in anesthesia preparatory time for the first cases of the day.
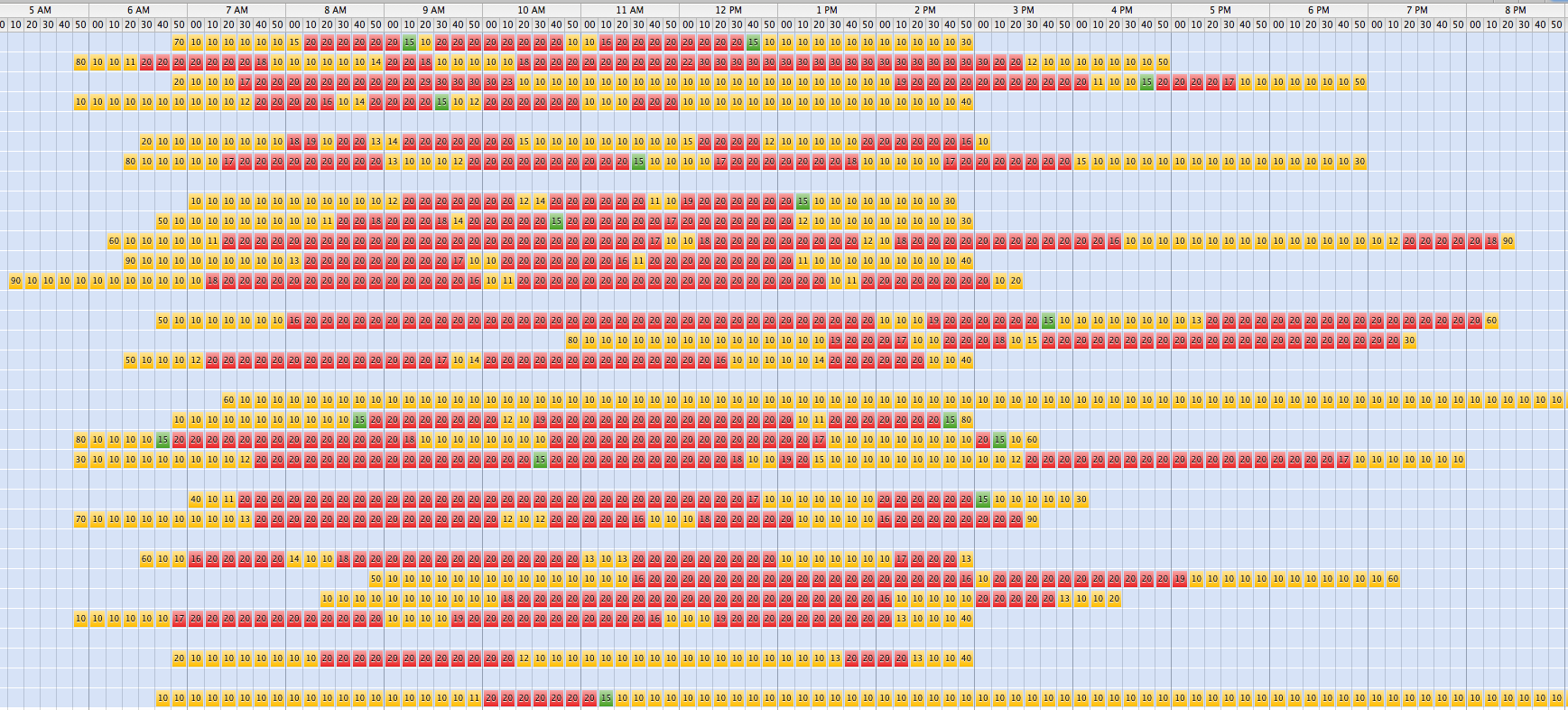
For a different graphic view of crna employee time paid vs crna down time see the following graphs. Each red square represents a 10 minute period during which 100% of the time the CRNA is clocked in she’s actually involved with a case (generating revenue) as indicated on an anesthesia record. Green represents less than 100% of the 10 minutes (1-10). Yellow means that the CRNA was being paid a salary but not bringing in revenue.
Capacity Utilization breakdown in 10 minute sections: working, CRNA idle while paid for working, 50% idle, white gaps are idle
Actual schedule: (notice that some CRNAs are idle, doing little to no work, the entire day)
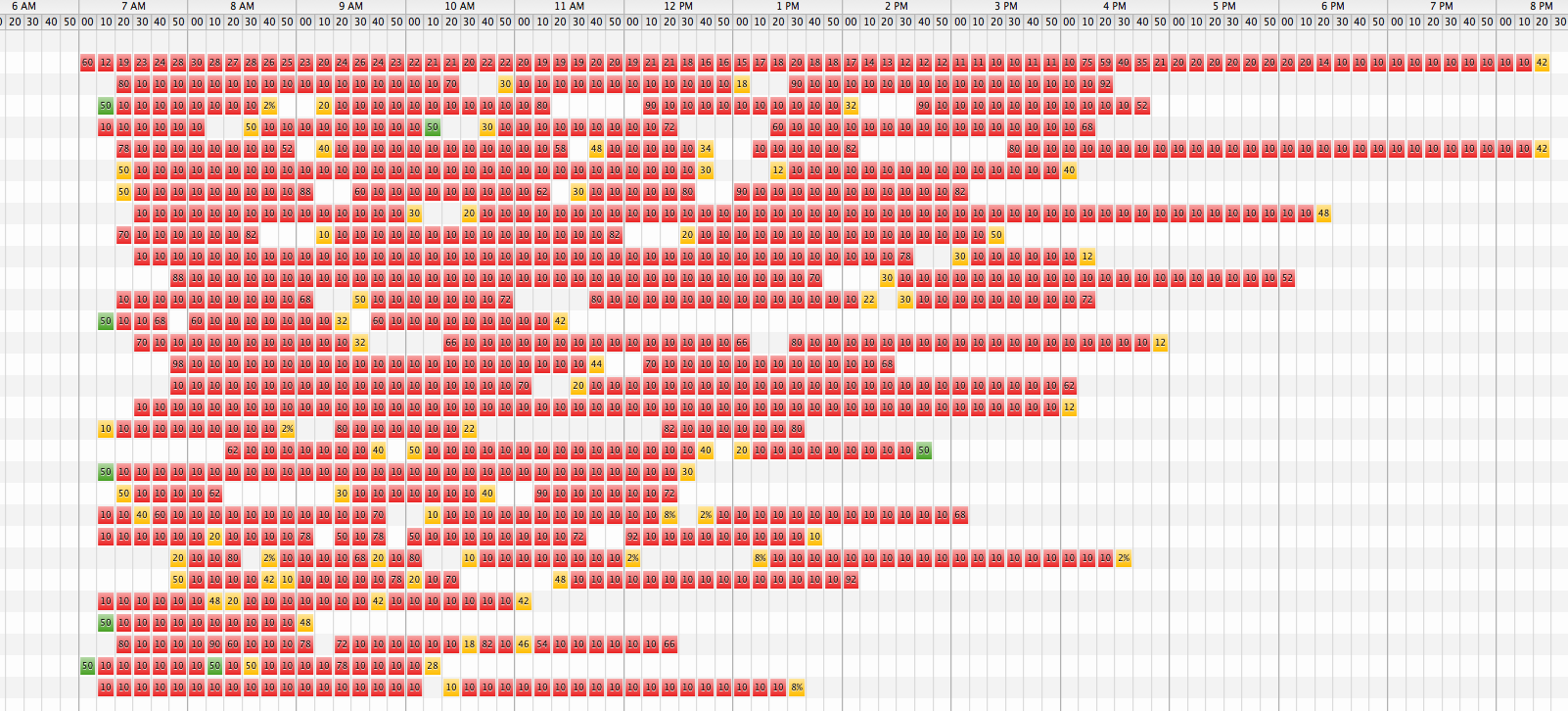
versus optimized: Below is a detailed plot of potential CRNA usage in the green graph above. Gaps in the schedule permit a particular CRNA to cover more than one room, thereby decreasing the total number needed (cumulative need shown in green graph above). Re-organizing the case schedule to ‘smooth’ CRNA usage during the day would decrease the number needed even more, but could affect other resource usage. The option to hire CRNAs for half days during peak need time is also an option.
CRNA hours billed vs paid in theoretical optimized schedule
Each line represents an OR room. The CNRAs in the bottom ‘optimal’ graph move from room to room with cases as needed to keep the surgeon busy, hence there are 30 rooms (lines) used instead of the 26 rooms (lines) in the top graph. The CRNAs in the top (actual, non-optimized schedule) tended to stay in one room (lots of idle time) instead of being optimally reassigned to other rooms with cases. As you can see, in the top graph there are long stretches of yellow squares (idle time) between red squares for many CRNAs. The bottom ‘optimized’ graph also has an extra 6 hour neuro case that I moved forward (not included in top graph) from later that night.
CRNAs often work a set number of hours a week (not per day). The trick is to have them working while they are present, and not waiting on cases. .These two graphs relate to my blog when PUNs equal CUEs which discusses FTEs. Tracking and effectively scheduling CRNAs can bring the ratio of CUE/PUN closer to 1. Scheduling surgeons well throughout the day also decreases their sTOT (CUE/PUN closer to 1). Both can be accomplished simultaneously as shown by the surgeon’s graph for this same optimized day: Wasting surgeons’ time.
Notice that the maximum amount of CRNA hours working at any one time in the optimized schedule is closer to 25, less than the 28 that were hired for the actual non-optimized schedule. This maximum load is from 8 am to 9 am which means that more cases are being completed earlier in the day. Compare that to the actual schedule which had it’s maximum usage between 10 am and 1 pm with only 18 -19 CRNA hours being in use at that time. Many of these extra early starts are due to preparation of a second (flip) case while the surgeon is still working on his first case of the day.
The maximum number of CRNAs can be reduced by covering 2 rooms with only 1 CRNA. Depending on the type case and surgeon, a fast CRNA can cover the same surgeon sequentially in two rooms, thus decreasing the total number of CRNAs needed. Increased pay (or other compensation) would be a good incentive for the CRNA to discover ways to quicken turnover. This applies to anesthesiologists as well; if on salary, a differentiation in pay is a good incentive to discover ways to quicken turnover. A corollary of this is that you should put slow CRNAs and anesthesiologists on long cases or on cases where it is not feasible for other reasons to have the anesthetist cover more than one room at a time.
The optimized case schedule is pretty much over between 4 and 5 pm while the actual non-optimized schedule drags on. Significant overtime pay can be saved by optimizing the cases. As for CRNAs, 24 were clocked in by 7 am in the actual schedule, with 14 being clocked in by 6 am or earlier, so there wouldn’t be much, if any, increase in time sheets on the front part of the day, but a significant decrease later in the day. Depending on how many cases you want to complete early, you could shift the schedule to decrease the maximum CRNA usage while not increasing the surgeon total time in the OR. The surgeons could come in a later, but still have a much shorter total stay. The fact that many surgeons do not arrive in time to take advantage of as early a start as possible leads one to conclude that they may be more interested in total time in the OR and the ability to finish their cases by a certain time of day. The early start could be just an attempt to finish early, but it is not the only way to finish early.
There are many considerations in optimizing the case load schedule in a particular hospital. What works for one won’t for another. Staggered start times also should be considered. Anyone who has worked in a busy OR is aware of the 8 am (or 7 am) OR congestion from trying to start too many cases at the same time. The effects can be similar to the morning rush hour traffic jam with everyone losing time. Again, it may not be the early start time that the surgeon most wants, but a shorter total time in the OR.
Reference for total CRNA usage during non-optimized schedule:

CRNAs employed buy not working
[Note that the scale for the upper and lower graphs are different]
The top graph shows times from the anesthesia records—the times that the CRNAs were doing cases (revenue for the anesthesia group).
The bottom graph shows the times the CRNAs were at the facility and being paid (expense for the anesthesia group). The red part of the graph shows how many extra CRNAs present that were not needed during the peak hours in the non-optimized schedule. This was not known by the hospital nor anesthesia group manager. Click on the link for more details: https://ortimes.org/2010/01/17/do-you-know-where-your-crnas-are/