Tags
- accounting
- administration
- Ambulatory Surgical Center
- anesthesia
- anesthesia residency
- anesthesiologist
- anesthesiology
- ASC
- board of directors
- board of directors data analysis
- business
- CEO
- cfo
- chairman
- cmo
- concept graph
- concept map
- constraints
- constraint theory
- COO
- cost accounting
- CRNA
- decisio
- decision algorithm
- deparment chairman
- dissatisfaction
- emotional intelligence
- finance
- flipping
- flip room
- FTE
- fungibility
- healthcare reform
- healthcare systems analysis
- healthcare systems engineering
- hospital
- hospital patient flow
- incentives
- information technology
- legal risk
- nurses
- operating room
- operating room efficiency
- operating room productivity
- operating theatre
- operations m
- operations management
- OR
- OR scheduling
- OR throughput
- PACU
- preOP
- revenue sharing
- risk
- risk management
- room flipping
- satisfaction
- schedule
- scheduling
- spc
- sqc
- surge
- surgeon
- surgery
- surgical case
- systems analysis
- systems engineering
- theory of constraints
- throughput
- throughput accounting
- toc
- TOT
- turn over time
- vice chairman
Tag Archives: OR
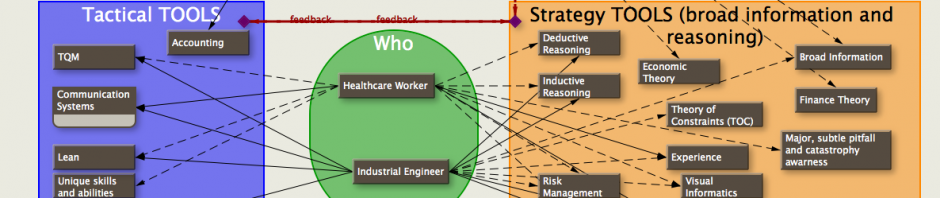
OR scheduling concept map (concept diagram)…
A few years ago I diagrammed several concepts involved in scheduling an OR onto this graph. The intent was to take advantage (or nullify disadvantages) of characteristics of individual surgeons and anesthetists. The interplay of these concepts and individual factors … Continue reading
Posted in anesthesiologist, concept graph, concept map, healthcare reform, scheduling, surgeon
Tagged anesthesia, concept graph, concept map, COO, OR, scheduling, surgery
2 Comments
getting your hands dirty…
Sometimes, to get what you want, you have to jump in and get your hands dirty… It’s been a month since my last post, a series of posts dealing with ‘what ifs’ and some simple simulations dealing with scheduling OR … Continue reading
Posted in anesthesiologist, CEO, healthcare reform, scheduling, Uncategorized
Tagged cfo, healthcare reform, healthcare systems analysis, OR, scheduling
Leave a comment
absolute loss of time…
In medicine, almost nothing is absolute. Absolutes are strictly enforced, unless the person who decided that it was an absolute changes his mind. In the narrow world of OR throughput, this is an important factor why surgeons (and anesthesiologists) should … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged decision algorithm, OR, surgeon
Leave a comment
coffee and donuts…. time for a break
Oh what fun… This is just one of many factors affecting turnover time (TOT). For the sake of smaller graphs and clarity, I’m showing only the times till anesthesia induces the patient to show the comparison of … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesiology, OR, scheduling, theory of constraints
2 Comments
difficulties with start times and TOT in the OR…
The following are excerpts from a discussion concerning Turn-Around-Time (TOT) in the OR. They relate to my recent posts on scheduling, and show the complexity/difficulty in defining the problems and solving them: ____ she: There are benchmarks out in the … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, decisio, OR, scheduling, surgical case
Leave a comment
micro real options in the OR…
One advantage of performing virtually identical cases—such as specialty ORs (cataract surgery would be an example) is that the room setup is virtually identical and a great deal of time can be saved (or avoided) by being able to put … Continue reading
Posted in anesthesiologist, healthcare reform, scheduling, surgeon
Tagged COO, finance, OR, schedule, scheduling
Leave a comment
Big Bwana and little bwana…
Everything in the below graph is adjustable (and is derived from less data than is normally collected in an OR). It’s quite useful when deciding how to create your portfolio of surgeons, anesthesiologists, or nurses to limit the short-comings, and … Continue reading
Posted in anesthesiologist, board of directors, CEO, healthcare reform, scheduling, surgeon
Tagged anesthesia, COO, finance, healthcare reform, healthcare systems analysis, OR, surgery, surgical case
Leave a comment
the cost of late surgeons… and the revenue from early surgeons
The purple bars represent the time saved for nursing staff and anesthesia if there is a policy for the surgeon to be ready to cut 30 minutes (adjustable) before the scheduled start of cases in the morning. The effects of … Continue reading
Visual analytics for an OR case…
Visual analytics for an OR case: Lots of information if you understand the code…. You can tell whether surgery, anesthesia, or the hospital personnel are on top of things and you can compare differences in techniques with resulting effects … Continue reading
Posted in anesthesiologist, scheduling, surgeon
Tagged anesthesia, COO, OR, surgeon, surgery, surgical case
Leave a comment
