See also: staffing anesthesiologists…the law of unintended consequences
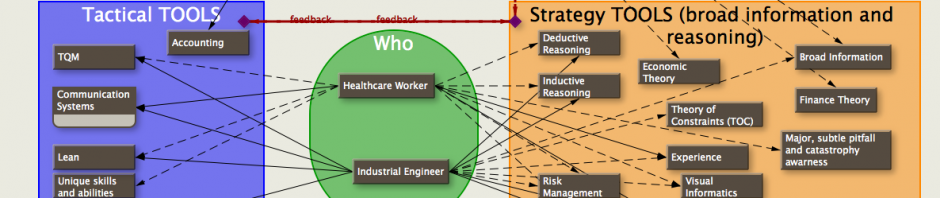
I’m emphasizing anesthetists as the fungible commodity (since they can be more readily fungible, and expensive), however it could be anything such as nurses, surgeons, equipment, OR rooms, etc. The existence of similar type cases, availability of more than one surgeon to work on any particular patient, residents, PAs, duplication of equipment or alternative equipment for any particular procedures, even alterating the sequencing of parts of particular cases can be used to expedite the flow of patients through the OR (and presumably the positive cash flow) and/or decrease the time required so that the participants (surgeons) can do office hours or surgery elsewhere for even more income. Every OR is different so it’d be almost impossible to construct a software program that could schedule all the cases and still make the participants happy. What you can do, though, is to educate the personnel in the OR in how to take advantage of options, and create tools that helps clarify these options (and results) that they can make.
After a good bit of theorizing, and several days of running scheduling simulations, I’ve come to the following conclusions:
Scheduling facts…
Fungibility is a good thing. Fungible implies that one object can take the place of another. Ideally, anesthetists are fungible: any anesthetist can do any case.
Some OR rooms are fungible—any case can be done in the room. The cysto room isn’t very fungible, neither are many OB surgical suites (mostly due to location).
Surgeons are the least fungible. For a given case, you’re pretty much stuck with one surgeon as a choice for that patient’s case (training facilities are different).
People, in general, are more fungible than OR rooms. It is easier to move people around than OR rooms with their setups.
All the above are reasons that in a crowded OR, if you optimize the total time in the OR for the surgeons, you’ll also optimize the total time in the OR for the anesthesiologists if the main purpose is to do as many cases as quickly as possible while utilizing every available OR room.
Also,
You can decrease the total number of anesthetists and still shorten the surgeons’ total OR times, but the workdays will last longer and the surgeons will have less choice on the time of day they work. This can, however, significantly increase the anesthetists’ income.
Letting surgeons schedule cases whenever they want is very costly for anesthesia and the OR. For the hospital, extra expense incurred in the OR by catering to surgeons may be recouped by revenue from other services and labs for the patient. Anesthesia has no such benefit and only suffers expense unless they have another source of revenue during the time gaps such as patients on an active pain service they can tend to.
If you have anesthetists who aren’t fungible, you decrease your options. Total down time for anesthesia, surgeons, and the hospital will increase. An anesthestist who does only one type of case is a liability.
Surgical groups which have members who can work on each other’s patients, and whose members are in surgery at the same time, increase the options for scheduling cases for fast turnover. Fungible surgeons are handy, but rare. I’ve seen it in OB groups, a neurosurgical group, and some urology groups.
An OB operating room attached to the main OR so that non-OB cases can be done in the OB rooms, and OB cases can be done in the non-OB rooms, is much more productive than an OB theatre separate from the main OR. Also, the OB surgical team will stay more up-to-date with the main OR’s standard guidelines for sterility and techniques when having to work with the main OR surgery nurses.

Pingback: ORTimes